Gail Slap, MD,
Elizabeth Goodman, MD,
Bin Huang, MS
1From the Division of Adolescent Medicine, Department of Pediatrics, Children’s Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, Ohio.
2001
ABSTRACT
Objective. Depression, impulsivity, and aggression during adolescence have been associated with both adoption and suicidal behavior. Studies of adopted adults suggest that impulsivity, even more than depression, may be an inherited factor that mediates suicidal behavior. However, the association between adoption and adolescent suicide attempts and the mechanisms that might explain it remain unknown. The objective of this study was to determine the following: 1) whether suicide attempts are more common among adolescents who live with adoptive parents rather than biological parents; 2) whether the association is mediated by impulsivity, and 3) whether family connectedness decreases the risk of suicide attempt regardless of adoptive or biological status.
Methods. A secondary analysis of Wave I data from the National Longitudinal Study of Adolescent Health was conducted, which used a school-based, clustered sampling design to identify a nationally representative sample of 7th- to 12th-grade students, with oversampling of underrepresented groups. Of the 90 118 adolescents who completed the National Longitudinal Study of Adolescent Health in-school survey, 17 125 completed the in-home interview and had parents of identified gender who completed separate in-home questionnaire. The subset of adolescents for this study was drawn from the in-home sampling according to the following criteria: 1) adolescent living with adoptive or biological mother at the time of the interview, 2) adolescent had never been separated from mother for more than 6 months, 3) mother was in first marriage at the time of the interview, and 4) the adoptive mother had never been married to the adolescent’s biological father. Of the 6577 adolescents in the final study sample, 214 (3.3%) were living with adoptive mothers and 6363 (96.7%) were living with biological mothers.
Variables. The primary outcome measured was adolescent report of suicide attempt(s) in the past year. Other variables included in the analyses were sociodemographics characteristics (gender, age, race/ethnicity, family income, parental education), general health (self-rated health, routine examination in the past year, need for medical care in the past year that was not obtained), mental health (depressive symptoms, self-image, trouble relaxing in the past year, bad temper, psychological or emotional counseling in the past year), risk behaviors (cigarettes, alcohol, marijuana, sexual intercourse ever, delinquency, physical fighting in the past year, impulsive decision making), school-related characteristics (grade point average, school connectedness), and family interaction (family connectedness, parental presence, maternal satisfaction with parent–adolescent relationship).
Data Analysis. Univariate analyses were used to compare adoptees versus nonadoptees, suicide attempters versus nonsuicide attempters, and adopted suicide attempters versus nonadopted suicide attempters on all variables. Variables that were associated with attempted suicide were entered into a forward stepwise logistic regression procedure, and variables that were associated with the log odds of attempt were retained in the model. The area under the model’s receiver operating characteristic curve was calculated as a measure of its overall performance. After the association of adoption with attempted suicide was demonstrated, the potential mediating effect of impulsivity was explored by adding it to the model. The same procedure was followed for any variable that was associated with adoption in the full sample or the subsample of suicide attempters. To determine whether any variable in the model moderated the association between adoption and suicide attempt, the interaction term for that variable × adoption was forced into the model.
Results. Adoptees differed significantly from nonadoptees on 4 of 26 variables. They were more likely to have attempted suicide (7.6% vs 3.1%) and to have received psychological or emotional counseling in the past year (16.9% vs 8.2%), and their mothers reported higher parental education and family income. Attempters differed significantly from nonattempters on all variables except for age, race/ethnicity, parental education, family income, and routine examination in the past year. On logistic regression, 9 variables were independently associated with attempted suicide: depression (adjusted odds ratio [AOR]: 3.41), counseling (AOR: 2.83), female gender (AOR: 2.31), cigarette use (AOR: 2.31), delinquency (AOR: 2.17), adoption (AOR: 1.98), low self-image (AOR: 1.78), aggression (AOR: 1.48), and high family connectedness (AOR: 0.60). The receiver operating characteristic curve for the model had an area of 0.834, indicating performance significantly better than chance. The AOR for adoption did not change when parental education, family income, and impulsivity were forced into the model. None of the interaction terms (adoption × another risk factor) demonstrated a significant effect.
Conclusions. Attempted suicide is more common among adolescents who live with adoptive parents than among adolescents who live with biological parents. The association persists after adjusting for depression and aggression and is not explained by impulsivity as measured by a self-reported tendency to make decisions quickly. Although the mechanism underlying the association remains unclear, recognizing the adoptive status may help health care providers to identify youths who are at risk and to intervene before a suicide attempt occurs. It is important to note, however, that the great majority of adopted youths do not attempt suicide and that adopted and nonadopted youths in this study did not differ in other aspects of emotional and behavioral health. Furthermore, high family connectedness decreases the likelihood of suicide attempts regardless of adoptive status and represents a protective factor for all adolescents.
Studies of the psychosocial function of adopted adolescents vary widely in their methods, findings, and interpretations. A 1998 review of the literature1cites 7 studies that demonstrate no differences between adopted and nonadopted adolescents,2–8 15 that demonstrate poorer adjustment among adopted adolescents,9–23 and 3 that demonstrate better adjustment among adopted adolescents on at least some variables.24–26 Much of the disagreement is attributable to differences in the populations of adopted youths that are studied and the control groups with which they are compared. For example, adopted and nonadopted subjects differ more when drawn from clinical rather than community populations.27–30 Subjects who are adopted in late childhood differ more from nonadopted subjects than do subjects who are adopted in infancy.29,31–33 Late-adopted subjects who were neglected during early childhood demonstrate more psychosocial difficulty during adolescence than do late-adopted subjects who were well cared for.29
The greatest controversy in the literature comparing adopted and nonadopted adolescents rests with the nature versus nurture interpretation of the reported differences. Although the study of adopted individuals has been an important strategy for exploring the genetic and family-associated environmental factors related to psychiatric disorders, its focus has been on the comparison of adoptive and biological relatives of adoptees rather than on the comparison of adoptees and nonadoptees. Consequently, findings that support an association of a given mental health disorder with family genetics rather than with family environment do not necessarily indicate that adoption is a risk factor for the disorder.
In an important adoption study designed to explore the role of genetics and family environment in the cause of mood disorders, Wender et al34 found significantly higher rates of unipolar depression, suicide, and attempted suicide among the biological rather than the adoptive relatives of adult subjects with mood disorders. The suicide rate among the biological relatives of subjects with a history of panic-type behavior or an impulsive suicide attempt was even higher, suggesting that impulsivity rather than depression may be the inherited factor that mediates suicidal behavior. In adolescents, impulsivity and aggression have been associated with both suicidal behavior35–38 and adoption,29,,35,36,39 and in both cases, gender and social environment modify the reported associations. Although these findings suggest an association between adoption and suicidal behavior, it is unknown whether adoptive status increases an adolescent’s risk for suicide attempt or completion.
This study used data from a large, national, school-based survey to test the primary hypothesis that attempted suicide is more common among adolescents who live with adoptive parents than among adolescents who live with biological parents. Second, we hypothesized that the association is mediated by impulsivity. Third, we hypothesized that one aspect of social environment—family connectedness—decreases the risk of suicidal behavior independent of adoptive or biological status.
METHODS
This study is based on data from The National Longitudinal Study of Adolescent Health (Add Health), the largest and most comprehensive survey of adolescents ever performed in the United States. Add Health was developed to examine the associations among health-related behaviors, social contexts, and physical environments. Data were collected through 4 surveys administered during Wave I (September 1994 through December 1995) and 2 surveys administered during Wave II (April 1996 through August 1996).24,,40The data for this study were drawn from the Wave I in-home sample.
Design of Add Health
Add Health used a school-based, clustered sampling design to identify a nationally representative sample of adolescents in the 7th through 12th grades of 134 schools, with specific oversamples.24 An in-school questionnaire was completed by 90 118 adolescents between September 1994 and April 1995. Students who completed the questionnaire plus students who did not complete the questionnaire but were enrolled in the schools were eligible for inclusion in an in-home sample. A random subset of 15 243 adolescents stratified by gender and grade were selected, and the 12 105 adolescents who completed in-home interviews composed the core in-home sample. In addition, special oversamples were drawn for the in-home survey to provide representation of ethnic minorities, in-school social networks, youths with physical disabilities, and siblings. The total in-home sample therefore consisted of the 20 745 adolescents who completed interviews between April 1995 and December 1995. A parent of each adolescent respondent, preferably the mother residing with the adolescent, was asked to complete a separate in-home questionnaire. Questionnaires were completed by 17 125 parents of identified gender between April 1995 and December 1995.24
The in-school survey was a self-administered paper questionnaire completed during a 45- to 60-minute class period on a designated school day. Students who were absent from the class were not given another opportunity to complete the questionnaire. To maximize confidentiality on the 90-minute in-home interview, the adolescent recorded all answers on a laptop computer. An interviewer read less-sensitive questions aloud to the adolescent. More-sensitive questions were prerecorded, and the adolescent listened to the audiotape through earphones and recorded the answer directly into the computer using audio-CASI technology.41 The 30-minute parent questionnaire was interviewer-assisted and op-scanned.24
Study Sample
The sample for this study was drawn from the Wave I set of 17 125 adolescents who completed in-home surveys and whose parents completed in-home surveys. An adolescent was considered eligible if he or she was living with his or her adoptive or biological mother at the time of the in-home interview and had never been separated from her for more than 6 months. If the adolescent’s mother had not completed the parent questionnaire, was not married at the time of data collection, or had been married more than once, then the adolescent was excluded from this study. An adolescent who lived with an adoptive mother was excluded if the adoptive mother had ever been married to the adolescent’s biological father. The final sample consisted of 6577 adolescents.
Each adolescent in the study sample was categorized as adopted or nonadopted according to information provided by the mother on the in-home questionnaire. The adolescent was considered adopted when the mother identified herself as the adoptive mother and nonadopted when the mother identified herself as the biological mother. The question, “Are you adopted?” was asked directly of adolescents on the in-school survey. However, because 25% of adolescents in Wave I did not complete the in-school questionnaire, the item was not used to define adoptive or nonadoptive status. It was included in the analysis to explore concordance between adolescent and maternal report of adoption. Of the 6577 adolescents in the study sample, 214 (3.25%) met criteria for the adopted group and 6363 (96.7%) met criteria for the nonadopted group.
Variables Included in the Analyses
All of the variables described below were derived from items on the in-home interviews of adolescents and their mothers. Some of the variables were derived from single items, whereas others were derived from groups of items. Participants who answered at least 75% of the items that composed a multi-item variable were included in the analysis of that variable. For these participants, the ratings for unanswered items in a multi-item scale were imputed from the mean rating of answered items in the scale. The study variables and their assigned categories are described below.
Suicide Attempt
Adolescents used a 5-point Likert scale to answer the question, “During the past 12 months, how many times did you actually attempt suicide?” Responses were dichotomized into no attempt versus 1 or more attempts. Add Health did not include a question about suicide attempts ever.
Sociodemographic Characteristics
Gender was identified by the adolescent on the in-school interview and validated by the in-home interviewer. Age was calculated from the date of interview and the date of birth. Racial/ethnic identity was indicated by the adolescent, with instructions to select the predominant affiliation if more than 1 was noted. The response was categorized as white non-Hispanic, black non-Hispanic, Hispanic, Asian/Pacific Islander, or other.
Family income was defined as the mother’s report of the total pretax income in dollars received by all household members in 1994, including dividends and welfare benefits. Report of 0 income was considered a missing response. Otherwise, reported income was adjusted for household size, compared with the 1994 threshold for poverty established by the US Census Bureau, and assigned to 1 of the following 5 classes: 1) <1.5 times the poverty threshold (a conservative estimate of substandard living conditions),42 2) 1.5 to <2.5 times threshold, 3) 2.5 to 4 times threshold, 4) 4 times threshold but less than the top 5% of 1994 household incomes, and 5) the top 5% of incomes.43
Parental education was determined from the mother’s response to the questions, “How far did you go in school?” and, “How far did your partner/spouse go in school?” The higher of the 2 answers was defined as parental education and was assigned to 1 of the following 5 categories: 1) did not graduate from high school and did not go to a vocational school instead of high school; 2) graduated from high school, received a high-school equivalency degree, or went to vocational school instead of high school; 3) went to vocational school after high school or went to college but did not graduate; 4) graduated from college; and 5) attended professional school after college graduation.
General Health
The adolescents were asked to rate their health on a 5-point Likert scale ranging from 1 (excellent) to 5 (poor). Self-rated health correlates with physical, mental, and social health. It is a valid and reliable indicator in adolescents and adults that differentiates individuals with and without chronic disease and is predictive of both the diagnosis of serious illness and the likelihood of survival.44,,45
Two items about general health care were included in the analyses. Adolescent responses to the question, “When did you last have a physical examination by a doctor or nurse?” were dichotomized as less than a year ago versus more than a year ago or never. Adolescent responses to the question, “Has there been any time over the past year when you thought you should get medical care, but you did not?” were dichotomized as yes or no.
Mental Health
Add Health contains 16 of the original 20 items that composed the Centers for Epidemiologic Studies Depression Scale (CES-D).46,,47 Two additional items from the CES-D were included in modified form. The internal consistency of the modified 18-item scale was excellent (Cronbach’s α = 0.87) and decreased when any item was dropped. The sum of these 18 items therefore was used to impute the full 20-item CES-D score after correcting for unanswered items. Each item was rated on a scale of 0 to 3. Potential CES-D scores thus ranged from 0 (no depressive symptoms) to 60 (maximum depressive symptoms).
In a study of 9th- to 12th-grade adolescents, Roberts et al47 found that the sensitivity and the specificity of the of the CES-D for the detection of major depressive disorders were maximized at scores of ≥24 for females and ≥22 for males. We used these cutpoints in the current study to create a dichotomous variable indicative of depression.
The self-image score was calculated as the mean of 6 items, each of which was rated on a 5-point Likert scale (Cronbach’s α = 0.85).40 Potential scores ranged from 1 (high self-image) to 5 (low self-image). Trouble relaxing in the past 12 months was assessed by a single item on the adolescent survey rated on a 5-point scale ranging from 0 (never) to 4 (daily). Bad temper was assessed by a single dichotomous item on the parent survey asking whether the adolescent had a bad temper.
Previous mental health care was assessed by dichotomized yes/no responses to the question, “In the past year, have you received psychological or emotional counseling?”
Risk Behaviors
Items that assessed cigarette use were combined to create a variable with the following 6 levels: 1 = never smoked, 2 = never smoked a whole cigarette, 3 = smoked a whole cigarette but not in the past 30 days, 4 = smoked at least a whole cigarette but less than a pack per week in the past 30 days, 5 = smoked at least a pack per week but less than a pack per day in the past 30 days, and 6 = smoked at least a pack per day in the past 30 days.
Items that assessed alcohol use were combined to create a variable with the following 5 levels: 0 = never had alcohol, 1 = had alcohol but not on more that 1 or 2 days in the past 12 months, 2 = had alcohol on more than 2 days in the past 12 months but less than every week in the past 12 months, 3 = had alcohol on 1 to 5 days a week in the past 12 months, 4 = had alcohol every day or almost every day in the past 12 months.
Items that assessed marijuana use were combined to create a variable with the following 5 levels: 0 = never used, 1 = used but not in the past 30 days, 2 = used 1 to 3 times in the past 30 days, 3 = used 4 to 29 times in the past 30 days, 4 = used 30 or more times in the past 30 days.
Sexual activity was assessed as a yes/no answer to the question, “Have you ever had sexual intercourse?” Delinquency was assessed as the sum of 15 items, each rated on a scale of 0 to 2 (Cronbach’s α = 0.84). Potential scores thus ranged from 0 to 30. Aggression was assessed by the question, “During the past 12 months, how often did you get into a physical fight?” Responses were dichotomized as “once” and “more than once” versus “never.” Impulsivity was assessed by the statement, “When making decisions, you usually go with your “gut feeling’ without thinking too much about the consequences of each alternative.” Responses were dichotomized as “strongly agree” and “agree” versus “neither agree nor disagree,” “disagree,” and “strongly disagree.”
School
Two variables that pertained to school were included in the analyses. The adolescent’s grade point average was the average of the self-reported letter grades at the last grading period in at least 2 of 4 core subjects: English, mathematics, history, and science. The grades were coded as follows: 1 = A, 2 = B, 3 = C, 4 = D or worse.
The school connectedness scale score was derived from 8 items, each rated on a 5-point Likert scale (Cronbach’s α = 0.75).40 Four items were rated on a scale of 1 to 5. The ratings for 3 items originally were coded by Add Health investigators on a scale of 0 to 4; these ratings were recoded on a scale of 1 to 5 to maintain consistency across items. The 8 item ratings were summed to yield a scale score with a potential range of 8 (low connectedness) to 40 (high connectedness).
Family
Three variables that pertained to family relationships were included in the analyses. The family connectedness scale score was derived from 13 items (Cronbach’s α = 0.83).40Each item was rated on a scale of 1 (low connectedness) to 5 (high connectedness). The ratings of 3 items were averaged to yield a mean. The 10 remaining items were divided into 4 subgroups, and the highest rating within each subgroup was selected to represent the subgroup. The 5 resulting ratings were summed to yield a scale score with a potential range of 5 (low connectedness) to 25 (high connectedness).
The parental presence scale consists of 7 items and has a potential range of 4 (low presence) to 22 (high presence)40; its method of construction precludes use of Cronbach’s α. Maternal satisfaction with the relationship with the adolescent was rated on a 5-point Likert-type scale. A higher rating reflected lower satisfaction.
Data Analysis
Sample weights were not applied in these analyses because fewer adopted than nonadopted subjects had been assigned weight variables by the Add Health investigators (90.2% vs 94.6%; P = .006). To decrease the likelihood of a type 1 error resulting from the unweighted analyses, we set statistical significance conservatively atP < .01. Nonparametric test phi coefficients were used as the measure of association for variables that violated assumptions of normal distribution.
Three sets of univariate analyses were performed. In the first set, adopted and nonadopted adolescents were compared on all variables. In the second set, adolescents who did and did not report suicide attempt(s) were compared. In the third set, adoptees and nonadoptees who attempted suicide were compared.
Variables from the second set of analyses that were associated with attempted suicide at P < .01 were entered into a forward stepwise logistic regression procedure to identify those that were independently associated with attempted suicide. Variables that were associated with the log odds of attempted suicide atP < .05 were retained in the model. To enhance comparability of the adjusted odds ratios, the continuous and ordinal variables in the model were converted to dichotomous variables. The CES-D score was dichotomized using Roberts’ criteria, as described above.47 The self-image, delinquency, and family connectedness scores were dichotomized as the highest tertile (low self-image, high delinquency, high family connectedness) versus the lower 2 quartiles. Cigarette use was dichotomized as levels 1 and 2 (never smoked or never smoked a whole cigarette) versus levels 3 to 6. The adjusted odds ratios and 95% confidence intervals are reported, and a receiver operating characteristic curve of the model was drawn by plotting the sensitivity (true positive rate) and 1-specificity (false-positive rate) at different cutpoints in the probability estimation of attempted suicide. The area under the curve was calculated as a measure of the overall performance of the model.48,,49
After the association of adoption with attempted suicide and its independence of depression and aggression was demonstrated, the potentially mediating effect of impulsivity was explored by adding it to the model. The same procedure was followed for any variable associated with adoption in either the full sample or attempt subsample. To determine whether any variable in the final model moderated the association between adoption and attempt, we forced into the model the interaction term for that variable × adoption.
RESULTS
Of the 6577 adolescents in the study sample, 214 (3.3%) lived with adoptive mothers and 6363 (96.7%) lived with biological mothers. At least 1 suicide attempt in the past year was reported by 213 (3.3%) of the 6577 participants.
Adopted and nonadopted adolescents differed significantly on 4 variables: attempted suicide, parental education, family income, and mental health counseling in the past year. Sixteen adopted adolescents (7.6%) and 197 nonadopted adolescents (3.1%) reported suicide attempt(s) in the past year (P< .001). Mean parental education was 3.6 ± 1.2 for the adopted group and 3.2 ± 1.2 for the nonadopted group (P = .0001). Mean family income level was 3.1 ± 1.2 for the adopted group and 2.7 ± 1.1 for the nonadopted group (P = .0001). At least 1 parent with a professional degree was reported by 73 adoptive mothers (34.1%) compared with 1238 biological mothers (19.5%;P < .001). Household income in the top 5% was reported by 21 adoptive mothers (9.8%) compared with 295 biological mothers (4.6%; P < .001). Counseling in the past year was reported by 36 adopted adolescents (16.9%) and 521 nonadopted adolescents (8.2%; P < .001). There were no significant differences between the adopted and nonadopted groups on any other variables.
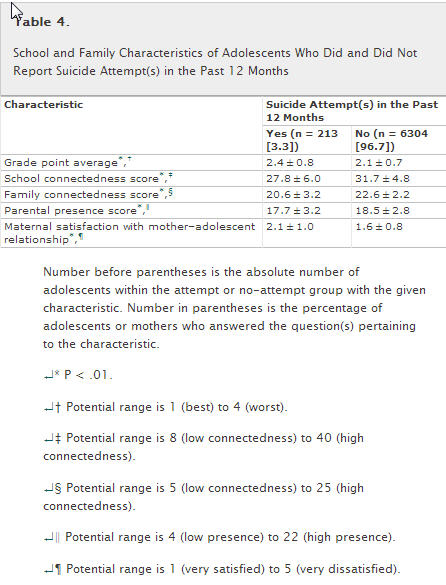
The univariate analyses comparing adolescents who did and did not report suicide attempt(s) in the past year are summarized in Tables 1 to 4. The groups differed significantly on all variables except for age, race/ethnicity, parental education, family income, and routine physical examination in the past year. Adolescents who attempted suicide, compared with those who did not, were more likely to be female (67.6% vs 49.1%) and adopted (7.5% vs 3.1%). They were more likely to rate their general health status as fair or poor and to report that they had not received needed medical care. Attempters had higher CES-D scores, were more than 5 times as likely to have scores consistent with depression, had lower self-image, and reported more trouble relaxing than did nonattempters. Attempters were more than 4 times as likely as nonattempters to have received mental health counseling in the past year. They were more likely to report all risk behaviors, including use of cigarettes, alcohol, and marijuana; sexual intercourse; aggression; impulsivity; and delinquency. Attempters reported poorer school performance, school connectedness, family connectedness, and parental presence than nonattempters. Mothers of attempters were more likely to rate their adolescents as bad-tempered and to report dissatisfaction with the mother–adolescent relationship than were mothers of nonattempters.
Table 1.
Sociodemographic Characteristics of Adolescents Who Did and Did Not Report Suicide Attempt(s) in the Past 12 Months
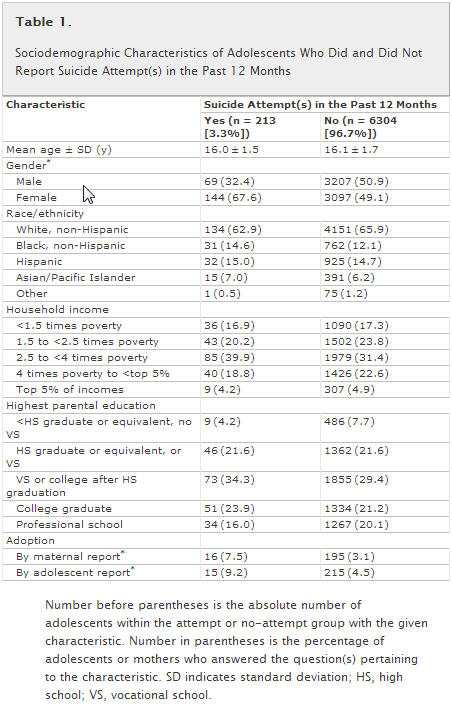
Table 2.
General and Emotional Health Characteristics of Adolescents Who Did and Did Not Report Suicide Attempt(s) in the Past 12 Months
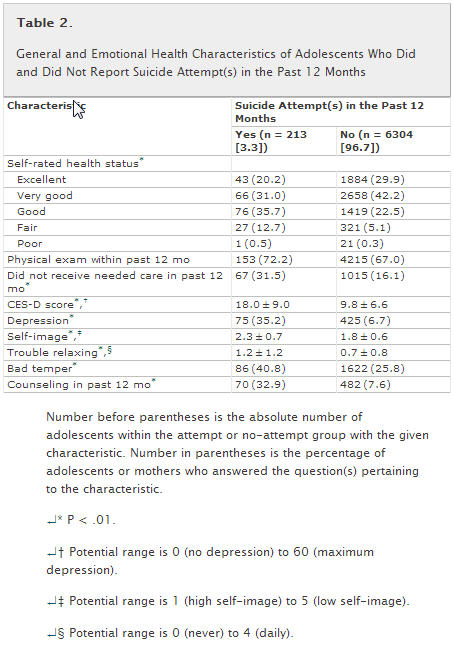
Table 3.
Risk Behaviors of Adolescents Who Did and Did Not Report Suicide Attempt(s) in the Past 12 Months
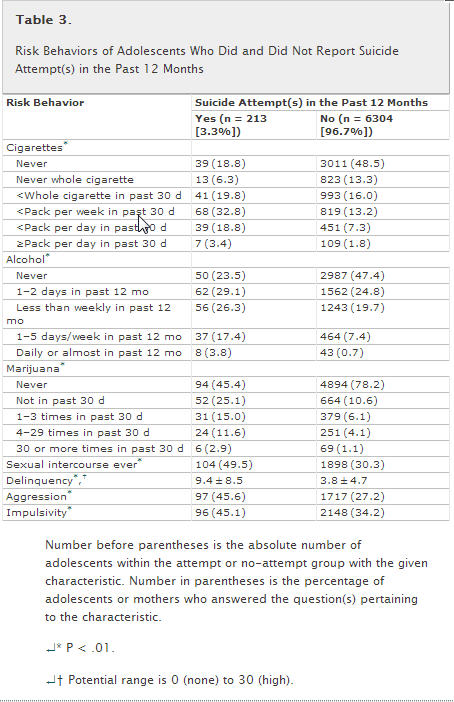
Table 4.
School and Family Characteristics of Adolescents Who Did and Did Not Report Suicide Attempt(s) in the Past 12 Months
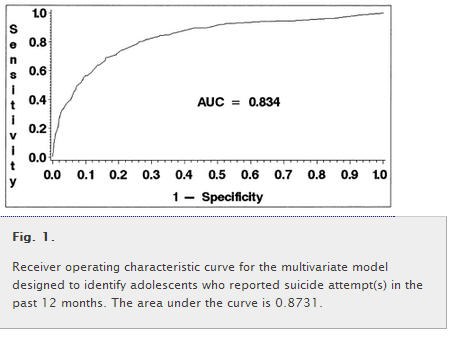
The 19 variables that were associated significantly with suicide attempt in the past year were entered into the forward stepwise logistic regression analysis. Of the 9 variables that composed the final model (Table 5), the following 8 increased the likelihood of suicide attempt: depression, mental health counseling in the past year, female gender, cigarette use, delinquency, adoption, low self-image, and aggression. One variable, high family connectedness, decreased the likelihood of attempted suicide. The receiver operating characteristic curve for the model, shown in Fig 1, had an area under the curve of 0.834.
Table 5.
Adjusted AOR and 95% CI of Variables That Composed the Stepwise Logistic Regression Model Designed to Identify Adolescents Who Reported Suicide Attempt(s) in the Past 12 Months
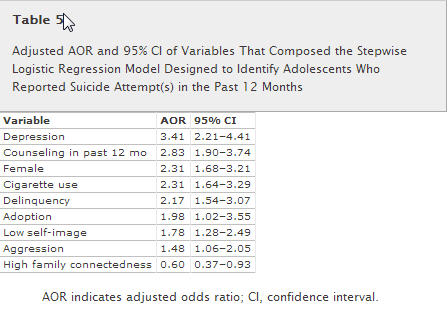
Fig. 1.
Receiver operating characteristic curve for the multivariate model designed to identify adolescents who reported suicide attempt(s) in the past 12 months. The area under the curve is 0.8731.
The addition of impulsivity, parental education, and family income to the model did not change the adjusted odds ratio of adoption. Comparison of adoptees and nonadoptees who attempted suicide revealed significant differences in only 2 variables, CES-D score (P = .005) and self-esteem score (P = .05), both of which were retained in the final model. None of the interaction terms (adoption × another risk factor) demonstrated a significant effect on the logistic model.
DISCUSSION
The results of this study indicate that attempted suicide is more common among adolescents who live with adoptive parents than among adolescents who live with biological parents. The study population intentionally was limited to adolescents who were living with their adoptive or biological mothers and who had not been separated from their mothers for longer than 6 months. Furthermore, because the participants’ mothers were in first-time marriages, it is likely that most of the participants had not experienced parental divorce and were living in 2-parent households. The adopted and nonadopted groups therefore were matched for 3 variables that have confounded many studies of adopted youths: family structure, parental divorce, and mother–child separation. Other important aspects of adoption, such as the child’s age at which it occurred or whether the adoptive parents were biologically related to the child, were not included in the Add Health data set. Variables such as these therefore remain key targets for the future study of suicide attempts among adopted youths.
The results of the current study support the primary hypothesis that adoption is associated with attempted suicide but do not support the secondary hypothesis that the association is mediated by impulsivity. However, it is important to remember that the Add Health survey did not include a validation of impulsivity. The CES-D, which is a validated measure of depression, showed much better discrimination between participants who did and did not attempt suicide than did the nonvalidated measures for impulsivity and aggression. Perhaps in-depth interviews designed to elicit self- and/or parent perceptions of impulsive or aggressive behavior would have yielded different results. Conversely, previous studies indicated that depression is a stronger and more consistent correlate of attempted suicide among adolescents than is either impulsivity or aggression.35,,36,3850–52
The study results do support the third hypothesis that family connectedness decreases the risk of suicidal behavior regardless of adolescent adoptive or nonadoptive status. The association between family connectedness and adolescent suicide attempt was reported previously for the full Add Health sample, which includes a broad array of family structures.40 The demonstration of its continued association in the highly select subset analyzed in this study, as well as its independence of adoptive or nonadoptive status, emphasizes how important family connectedness is to adolescent well-being. The finding is supported by a 1997 study by Rosnati and Marta53that showed that it is the quality of the parent–adolescent relationship, rather than adoptive or nonadoptive status, that predicts adolescent psychosocial risk. Family function, defined and measured differently than the Add Health construct of family connectedness, also has been shown to be associated with adolescent suicide attempt,54other risk behaviors, and depression.55
In addition to depression, adoption, aggression, and family connectedness, the following 5 factors demonstrated independent associations with attempted suicide in this study: mental health counseling in the past year, female gender, cigarette use, delinquency, and low self-image. All have been reported previously to increase the risk of suicide attempt during adolescence. The rate of suicidal behavior is 3 times higher for adolescents who have received previous outpatient mental health care and 7 times higher for adolescents who have received inpatient care than for adolescents with no history of care.56–60The predominance of females compared with males among adolescents who attempt suicide is well documented and contrasts sharply with the predominance of males who complete suicide during mid- and late adolescence.61,,62 However, data from the 1999 National Youth Risk Behavior Survey of 9th- to 12th-grade students indicate that race/ethnicity may affect the association between suicide attempt and gender. Rates of suicide attempt were significantly higher among white non-Hispanic and Hispanic females than males but did not differ by gender among black non-Hispanic students. Among all racial/ethnic and grade-level subgroups, females were more likely than males to report serious consideration of suicide during the previous 12 months.61
Both cigarette use and delinquency have been associated with adolescent suicidal behavior, as well as with mood disorders and substance abuse.38,,54,5563–69 The inclusion of cigarette smoking in the final model of the current study, rather than alcohol or marijuana use, was surprising given extensive evidence supporting the role of substance abuse as an independent risk factor for suicide attempt and completion during adolescence. Although cigarette smoking in most studies is associated with both suicide attempt and substance abuse, it seems to be a marker of risk rather than an independent predictor of suicidal behavior.50,,51,62,6370–73 The discrepancy in the findings of previous studies compared with the current study may reflect the differences between the clinically derived samples of previous studies and the school-based Add Health sample of the current study. It is likely that the severity of both suicidal behavior and substance abuse is higher for adolescents who have a history of psychiatric inpatient and/or outpatient care than it is for adolescents who are attending school and living at home. It also is possible that the in-home setting of the Add Health survey interfered with adolescent disclosure of alcohol and other drug use.
Another discrepancy between the current and previous studies is the independent nature of the association between low self-image and suicide attempt. Low self-image has been demonstrated to be a more consistent association with suicidal ideation than with suicide attempt,50,,61,70,74 and it has not been found to predict suicide attempt independent of other variables. The persistent effect of low self-image in this study, after adjustment for well-established predictors of attempt such as depression, aggression, impulsivity, and family factors, suggests that the adolescents who reported attempt(s) in the past year may have had ongoing suicidal ideation at the time of the survey.
CONCLUSION
Suicide attempts are significantly more common among adolescents who live with married adoptive mothers than among adolescents who live with married biological mothers. The association between adoption and attempted suicide persists after adjusting for depression and aggression and is not mediated by impulsivity as measured by a self-reported tendency to make decisions quickly. Although the mechanism underlying the association remains unclear, adoptive status may help health care providers to identify youths who are at risk and to intervene before a suicide attempt occurs. It is equally important to note, however, that the great majority of adopted youths do not attempt suicide and that adopted and nonadopted youths in this study did not differ in other aspects of emotional and behavioral health. Furthermore, high family connectedness decreases the likelihood of suicide attempts regardless of adoptive status and represents a protective factor for all adolescents.
ACKNOWLEDGMENTS
There was no financial support outside the division for this study.
This research is based on data from the Add Health project, a program project designed by J. Richard Udry (PI) and Peter Bearman and funded by Grant P01-HD31921 from the National Institute of Child Health and Human Development to the Carolina Population Center, University of Carolina at Chapel Hill, with cooperative funding participation by the National Cancer Institute; the National Institute of Alcohol Abuse and Alcoholism; the National Institute on Deafness and Other Communication Disorders; the National Institute of Drug Abuse; the National Institute of General Medical Sciences; the National Institute of Mental Health; the National Institute of Nursing Research; the Office of AIDS Research, National Institutes of Health (NIH); the Office of Behavior and Social Science Research, NIH; the Office of the Director, NIH; the Office of Research on Women’s Health, NIH; the Office of Population Affairs, Department of Health and Human Services (HHS); the National Center for Health Statistics, Centers for Disease Control and Prevention, HHS; the Office of Minority Health, Centers for Disease Control and Prevention, HHS; the Office of Minority Health, Office of the Assistant Secretary of Health, HHS; the Office of Assistant Secretary of Planning and Evaluation, HHS; and the National Science Foundation. These data are not available from the author. Persons who are interested in obtaining data files from the National Longitudinal Study of Adolescent Health should contact Francesca Florey, Carolina Population Center, 123 West Franklin St, Chapel Hill, NC 27516-3997. E-mail:fflorey@unc.edu
We thank Yolanda Hill, MD, for her help with the literature review and Lynn McDermott for her secretarial support.
PDF and References: Adoption as a Risk Factor for Attempted Suicide During Adolescence




My head is killing me from our marathon drive to court the other day so please bear with me, but does this study include children adopted from foster care or does it focus on infant adoption?
I don’t think this study differentiated that, but the other one took that into account!